Tablet Scoring in Pharmaceuticals
An emerging concept in the pharma industry, Tablet Scoring in Pharmaceuticals refers to the breakage of a tablet to attain a desired efficacy dose. The investigation of tablet scoring is still at its infancy and its potential yet to be fully explored.
Tablets are generally scored for the following reasons:
(1) Facilitate administration. Several factors can influence a patient’s inability to swallow a large tablet: dysphagia or difficulty swallowing, patients in moribund state, age-related psychological changes, pediatric patients.
(2) Reduce cost and adjust dose. When a higher therapy dose is no longer needed, patients split tablets to save cost. The price variation among different tablet strengths is typically minimal. Requesting a higher dosage tablet strength in order to partition the tablets can be more economical to some patients.
(3) Facilitate dose alteration. Dose alteration involves changing the marketed dose to achieve a target dose, hence, dose tapering or dose titrating.
Dose tapering refers to starting a medication at a high dose and slowly decrease the dose to wean the patient out of the medication. Dose tapering is typically done to prevent the effect of medication withdrawal. Medical withdrawal often is associated to clinical adverse reactions. Dose titration refers to starting a medication at a low dose and slowly increasing the dose to the target level. Tablet splitting provides proper dosage in cases where slow dose titration and dose tapering are necessary, particularly with medicines that control the central nervous system.
(4) Overcome changes in insurance policies. This practice aligns with cost savings; the down turn of the economy has mas made it a more common practice. Some insurance companies have denied payments for lower-strength tablets, which requires patients to obtain a larger dosage and then split the tablets.
Out of specification tablets.
- Controlled release tablets have been designed to release the medication in a predictable manner over time. To accomplish this, a variety of methods have been employed. Some methods, such as the use of coated granules, may be suitable for tablet splitting. Other dosage forms, however, would have their designed features impaired by splitting. The difficulty in assessing the suitability of each controlled dosage form and the potential effect on their function makes it not favorable to partition these tablets.
- Non-robust tablets. Tablets with inadequate physical properties (e.g., low hardness, high friability) can crumble or shatter because of the brittleness property and/or low hardness values during splitting/partitioning. This can compromise the desired dose and may lead to product fragmentation and wastage.
- Inadequate dose. This can present serious clinical adverse reaction, particularly in the case in which a drug of narrower therapeutic index is used. Uneven split tablets may lead to administration of incorrect dose. Certain products, particularly potent compounds, are available commercially at doses of less than 1 mg. Splitting such smaller dose tablet can lead to dose inaccuracy, hence can pose serious clinical risks.
Controlled-release tablets should never be split. Altering these types of tablets can potentially allow immediate absorption of the full dosage, which can saturate the plasma level and lead to overdosing. This can pose a risk of serious adverse reaction.
- Similarly, splitting opioid tablets can result in dose inaccuracies and can be harmful to patients. In order to mitigate opioid abuse, several steps have been implemented by the FDA to ensure that companies reformulate their painkiller tablets in a way that will make it more difficult to alter the dose. The reformulation known as opioid abuse-deterrent formulations (ADFs), involves adding a blocking agent that will counter the effect of opioids if dissolved and injected. There are a few formulations for oxycodone (e.g., Targiniq ER) and other opioids that have been approved by the FDA that utilize the abuse-deterrent opioid formulation. To mitigate the opioid abuse crisis, these new formulations use specialized excipients that make it difficult to crush the tablets. Another strategy of abuse deterrence involves incorporating aversion properties into the formulation. For example, components that can produce unpleasant effects if the opioid tablets are manipulated.
Patients with complex dexterity issues, may have difficulty splitting tablets, either manually or with the use of a tablet splitter and with the use of other non-conventional objects used to partition tablets.
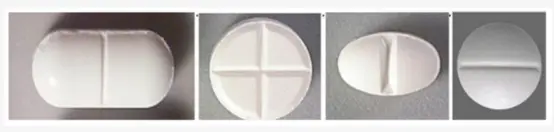
In some cases, tablets are partitioned unevenly, which can pose some compliance issues and minimize the reliance on the drug. Geometrical configurations of the tablet such as shape, size, thickness and curvature play a crucial role on the performance of the score lines. The depth of the score line can also be a contributing factor. Performance of score lines can be defined by breaking ease, uniformity of mass of subdivided tablets and loss of mass by the subdivision. For breaking ease, an in-vivo reference test and a routinely applicable in-vitro test need to be established. For the uniformity of mass of subdivided tablets, a requirement has recently been set by the European Pharmacopoeia. Loss of mass upon breaking can be limited to not more than 1%.
Tablet physical properties such as size, curvature and thickness, and the form and deepness of the score line as well as scoring techniques can affect the effectiveness of tablet splitting. To facilitate tablet splitting, recent studies have suggested the use of compression molding. Compression Molding is a semi-manual operation where tablets are formed by forcing the wet granulated blend into a mold to achieve tablets of desired shapes and sizes.
Tablet weights and uniformity of dose are interdependent. Uneven scored tablets can pose great clinical risk, especially when targeting a narrow therapeutic-toxic range. By contrast, tablets with wider therapeutic indices and longer half-life are more forgiving to uneven splitting.
In a nutshell, while there are cost benefits associated with tablets splitting/partitioning, this practice is extensively used for clinical reasons. In a larger perspective, using tablet splitting to reduce costs is limited by the number of products suitable for tablet splitting. The practice is largely dependent on the actions of pharmaceutical manufacturers for Tablet Scoring in Pharmaceuticals.
Factors that can influence tablet splitting practices include:
(1) the number of dosages available,
(2) tablet properties,
(3) tablets that require specialized excipients to target a modulated release profile, and
(4) storage conditions.
Patients should be able to split tablets easily, either by hand or with the use of a tablet splitter. To achieve the therapeutic and economic benefits from tablet splitting, patients need to be educated on the rationale and procedures of tablet splitting. Tablet splitting/partitioning has played a crucial role in modern medicine, as the ability to dose taper and dose titrate is important across therapeutic areas. Based on some accrued clinical data, some warning has been issued around the practice of tablet splitting/partitioning. According to clinical observations, approximately a third of the partitioned tablets fall outside of the recommended dosages by more than 15 percent.
Tablet Splitting: Regulatory Guidance
Weight and uniformity variation can expose a patient to:
(a) Drug underdose. This is a case of a patient who is continuously being exposed to a low (inefficacious) amount of a drug, hence under dosing. This can potentially create resistance to that drug, which can render the therapy ineffective. That may cause serious side effects, may prevent the drug from working properly, and/or may slow down the efficacy of the therapy.
(b) Drug overdose. This can be very harmful to patients, especially for high potency drugs.
The FDA guidance as it is written is similar to that of unscored tablets with added requirements to prevent risks associated with drug exposures upon administration about Tablet Scoring in Pharmaceuticals.
- All scored tablets should be stable at: 5 °C, 25 °C/60%RH, 40 °C/75%RH for up to 90 days. Stability studies should be performed in appropriate container closures.
- Scored tablets should be stable in pharmacy dispensing containers for up to 90 days 25 °C/60%RH.
- The label should encompass the therapeutic dose.
- Enteric coated tablets should not be scored.
- The physical characteristic criteria for scored tablets are similar to that of whole tablets.
- Scored tablet Content Uniformity and Uniformity of Dosage unit as specified in USP 37 chapter 905.
- Scored tablet Water Content as specified in in USP 37 chapter 921.
- Scored tablet Dissolution as specified in USP 37 chapter 711.
- Scored tablet Microbial Examination as specified in USP 61 and 62.